
In this article, I want to talk about deep stops and the on/off-gassing mechanism of our bodies during dives. This article is not meant to justify whether deep stops are a good or a bad thing, nor act as a guideline for your dives; rather, I wrote it to compile the information about tissue on-gassing, deep stops, and give a deeper insight into the science behind scuba diving and decompression theory.
Starting off, let's talk a little bit about the origins of deep stops - also known as Pyle stops, named after Richard Pyle. Richard Pyle was an American ichthyologist (a fish scientist) and a scuba diver. During his expeditions to retrieve certain specimens of fish, he would occasionally find himself at depths of up to 220 feet (About 70 meters), and upon ascents, he would have to allow air to escape the fish's swim bladder to prevent it from overexpanding and damaging its other internal organs. He would stop at around 125 feet (38 meters) and "temporarily insert a hypodermic needle into their swimbladder, venting off the excess gas": while on such a dive, his first decompression stop would be around 50 feet (15 meters), and the time he took to vent the swimbladder acted as an intermediate stop. Over time, he would come to realize he was feeling more fatigued on dives where he wasn't taking that intermediate stop. After this, he systemically incorporated those deep stops to his dives, and magically, it seemed like all his post-dive tiredness disappeared!
When Richard started spreading the word about deep stops, skeptical eyebrows were raised, since the primary belief was that the diver, once their bottom time was completed, should ascend as fast as possible to "get out of deep water as quickly as possible to minimize additional gas loading". It was only when he saw a presentation by Dr. David Yount (one of the creators of the Varying Permeability Model, or VPM) that Richard was able to equate his theory to a physiological mechanism: the VPM model considers the presence of "micronuclei", or "microbubbles" in our body at all times, and that preventing DCS would be tantamount to limiting the radii of those bubbles. One of the factors he considered was the rate of reduction in ambient pressure during an ascent: he argued that allowing more time between the bottom time and the first decompression stop by slowing the ascent rate and/or adding deeper stops would prevent those bubbles from expanding rapidly.
All the information compiled here justifying the origin of deep stops comes directly from a paper written by Richard Pyle, "The importance of Deep Safety Stops: Rethinking Ascent Patterns From Decompression Dives," published in the South Pacific Underwater Medicine Society (SPUMS) Journal Vol 27 No.2 June 1997
Whether deep stops are justified or not is not for me to say, but I would, regardless, like to present the subsequent research carried out on deep stops and explain, from a neo-haldanian point of view (think compartments), how they affect divers.
Before explaining further, it is important to understand compartments as a basic concept of decompression theory. If you'd like to read about them in more detail, you can check out this article.
The case against Deep Stops
The main argument against deep stops is as follows: during deep stops, although your fast compartments are off-gassing, the slower (and potentially intermediate) compartments are still on-gassing. Therefore, exposing yourself willingly to deep stops only increases your supersaturation levels and potential DCS risks throughout the dive. Now, although the argument is far from baseless, rather than throwing arguments right and left, let's look at some facts: I want to talk about 2 papers that cover deep stops: A paper published by Jean-Eric Blatteau in 2005 and a paper published by David J. Doolette of the Navy Experimental Diving Unit (NEDU) in 2011.
The paper published in 2005, written by Jean-Eric Blatteau, named "Bubble incidence after staged decompression from 50 or 60 msw: effect of adding deep stops" studied the post-dive effects of decompression models incorporating deep stops and compared it to the MN90 tables (Marine Nationale 90, the French decompression tables). Three different dive protocols were organized (each time comparing the MN90 plan to the new "experimental" plan incorporating deep stops):
- Protocol I with a bottom depth of 60 meters and starting deep stops depths of 27 meters.
- Protocol II consisted of a repetitive dive to a bottom depth of 50 meters, a surface interval of 3 hours, and starting deep stops at 18 meters.
- Protocol III, consisting of a single dive with a bottom depth of 60 meters, incorporating a shorter deep stop at 25 meters.
The divers were monitored for precordial bubbles with an interval of 30 minutes using Doppler sensors. The results in protocol III showed no difference between decompression models. For protocol II, the divers doing the deep stops showed severe bubbling, and for protocol I, one of the divers doing a deep stop had a DCS case. The researchers concluded that "The addition of deep stops requires careful consideration".
The second paper I want to talk about is titled "Redistribution of Decompression Stop Time from Shallow to Deep Stops Increases Incidence of Decompression Sickness in Air Decompression Dives", published by NEDU in 2011. In this paper, David Doolette, Wayne Gerth, and Keith Gault compared classical decompression algorithms to bubble models (that have deeper stops).
In practice, the researchers had the divers follow two different profiles: The "shallow profile", which prioritized shallow decompression stops, based on the VVAL-18 Thalmann algorithm schedule, while the "deep profile" had the depths redistributed to incorporate deeper stops according to the BVM(3) probabilistic decompression model. The dives were conducted on air, and the exact profile is as follows:
| Depths (m) | Shallow profile | Deep profile |
|---|---|---|
| 52 | 30 min | 30 min |
| 21 | 12 min | |
| 18 | 17 min | |
| 15 | 15 min | |
| 12 | 9 min | 18 min |
| 9 | 20 min | 23 min |
| 6 | 52 min | 17 min |
| 3 | 93 min | 72 min |
Out of 192 dives for the shallow profile, 3 instances of DCS were recorded (1.56%), while out of 198 dives for the deep profile resulted in 11 DCS cases (5.56%). Additionally, resting VGE (Venous Gas Emboli) grades were measured and were found to be consistently higher after the deep-stop dives compared to the shallower-stop dives. The paper concludes that "The practical conclusion of this study is that controlling bubble formation in fast compartments with deep stops is unwarranted for air decompression dives."
What happens during a deep stop?
Let's forget about bubble models for a second: for this part, I'd like to consider the compartmental side of it and observe how our tissues saturate and desaturate during a dive, and how adding a deep stop affects this "saturation". From what we have already talked about, we can guess what will appear: compared to the normal dive profile, the one incorporating deep stops will show the faster tissues less saturated and the slower tissues more saturated.
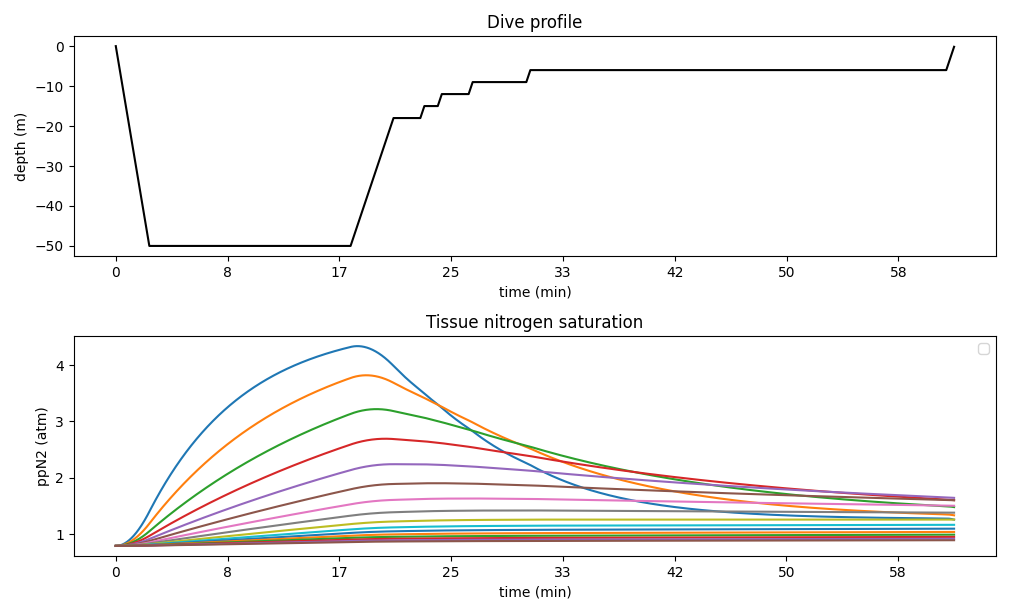
Nevertheless, let's illustrate this with an example of a decompression dive in which the diver descends to a depth of 50m for 15 minutes. For the sake of simplicity, the diver will use only air throughout the dive, with 40/80 as gradient factors in the ZH L-C model. The yielded plan using those settings is:
| 50m | 15:00 |
| 18m | 2:00 |
| 15m | 1:00 |
| 12m | 2:00 |
| 9m | 4:00 |
| 6m | 31:00 |
The ascent and descent aren't mentionned, but are taken into account. The chosen descent speed is 20m/min and the ascent speed is 10m/min. To monitor our tissues, we can graph their saturation level throughout the dive:
Now, let's add deep stops to this plan. To do that, we will use Richard Pyle's method:
- Compute the halfway depth between the bottom depth and the first stop, and add a stop there for two or three minutes.
- While the distance between the pyle stop and the first decompression stop is greater than 9m, repeat the process.
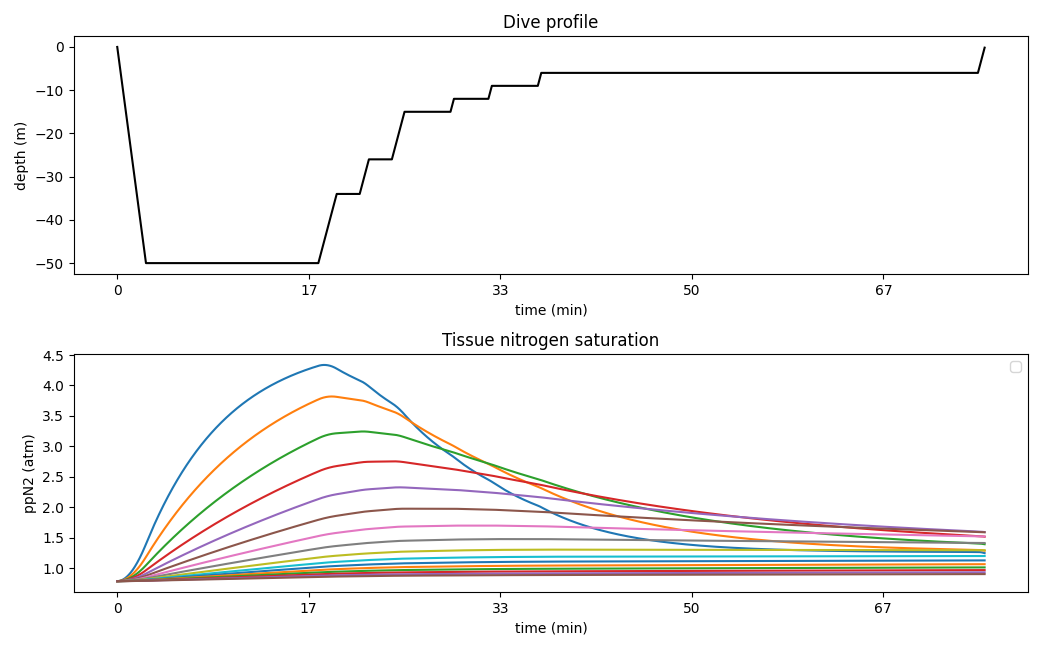
By using this method, we get an additional pyle stop at 34 and 26 meters (I chose to stay for 2 minutes only). It is important to recompute the decompression plan after taking the new stops into account: dive computers will do that automatically and in real time, but if we are using decompression software, we need to include those new stops. We can simulate the new decompression dive with deep stops by feeding the bottom plan to the planning software (the plan now consists of the bottom time at 50m for 15 minutes, followed by a 2-minutes stop at 34m, and a 2-minutes stop at 26m). The yielded plan is:
| 50m | 15:00 |
| 34m | 2:00 |
| 26m | 2:00 |
| 15m | 4:00 |
| 12m | 3:00 |
| 9m | 4:00 |
| 6m | 38:00 |
The parameters (ascent/descent speed, conservatism, etc...) are the same as the first plan. You might notice that although there is more total decompression time, the stop at 18m disappeared: this is normal as the deep stops acted as "deeper decompression stops". Because the distance between 26 and 15 meters is greater than 9 meters, it would be possible to add yet another pyle stop: for the sake of simplicity, we won't do that here. Once again, let's track the nitrogen saturation level of our tissues throughout the dive:
In both profiles, out of the 16 curves, the blue one (the one that rises faster during the on-gassing phase) represents the fastest tissue, with a half-time of 5 minutes; the orange-yellowish one (the second one to rise the fastest) represents the second fastest tissue, with a half-time of 8 minutes; and so on. During the bottom part of the dive, all curves saturate at a rate corresponding to their half-time. The difference between profiles arises when the diver begins their stops:
- In the first profile, because there are no deep stops, the diver starts their stop at a shallower depth, which allows all tissues to desaturate faster. Additionally, all compartments up to the 6-7th are properly off-gassing (if you look at the curves, the other are still slightly increasing even during the first decompression stop, which indicates on-gassing).
- In the second profile, as the deep stops force the diver to start their stop deeper, the first two compartments are off-gassing slightly slower, while all the other compartments are still on-gassing - we have to wait to hit the next stops for the subsequent compartments to start desaturating.
The difference between these two profiles has two main consequences: firstly, the medium to slow compartments present an overall higher total amount of oversaturation at the end of the dive. Secondly, the dive time is greater in the second profile due to the higher time to on-gas for those tissues, which then requires more decompression time.
Expanding a little bit more about nitrogen on/off-gassing, I previously wrote an article about optimizing safety stops and how those safety stops affect the nitrogen levels in our bodies. Without going into details too much, the conclusion was similar for shallow recreational dives: the fast tissues will benefit from off-gassing, while the slower tissues might still on-gas a little bit. Note: this is only valid for shallow recreational dives; otherwise, and especially at the end of decompression dives, shallow safety stops will off-gas all tissues. Similarly to deep stops, it depends on the tissue's current saturation level compared to the inert gas partial pressure at the current depth.
